Kim, Hyun Jung, Kim, Woon Young, Lee, Yoon Sook, Chang, Moon Seok, Kim, Jae Hwan, and Park, Young Cheol The Effect of Cranial Electrotherapy Stimulation on Preoperative Anxiety and Hemodynamic Responses. Korean Journal of Anesthesiology. 2008; 55(6): 657- 661. Download Article
Device
Alpha-Stim®
Key Variable
Preoperative Anxiety
Objective
To evaluate the effect of a specified treatment course with CES on patients’ preoperative anxiety levels when compared to sham treatment under the same experimental conditions in subjects meeting the inclusion and exclusion criteria.
Design
This was an IRB approved randomized, investigator-blind, clinical trial. The active CES device was set to “just below” 200 µA, where subjects did not feel a tingling sensation.
Primary Effectiveness Endpoint
The primary effectiveness endpoint was the change from baseline in the post-treatment scores on the Likert anxiety scale compared to the sham group at the end point of the study.
Key Inclusion Criteria
• Preoperative patients between the ages of 18-65 awaiting surgery under general anesthesia.
• Must meet the American Association of Anesthesiology Physical Classification Criteria 1 and 2.
Key Exclusion Criteria
• Pregnancy.
• Presence of implanted pacemakers, pumps or stimulators.
• BMI over 25, and having endocrinological, musculoskeletal, liver and kidney or vascular disorders.
• Individuals awaiting high anxiety procedures such as tumor removal or amputation.
• Individuals who were taking antidepressant and other psychotropic medications.
Protocol Summary
Detailed explanations for study purpose and procedures were provided to the patient and their families and consents were obtained the night before the surgery. They were told that they will be held for 20-30 minutes in the pre-surgical waiting area and they will either receive or not receive CES and what sensation to expect from CES pretreatment in order to reduce anxiety.
All subjects were given glycopyrrolate 0.2 mg IM as a premedication about one hour before induction of anesthesia. They were brought to the waiting area to be evaluated by the same anesthesiologist who visited them the night before. They were asked about their level of anxiety and blood pressure and pulse rate was measured as a physiological index of anxiety. Anxiety was rated using a Likert Scale measuring the subjective experience of anxiety on a scale of 1 (low) to 5 (high). Subjects were randomly assigned to either a control group (n=30) who received supportive nursing care or a CES group (n=30) who received a 20 minute CES pretreatment in the operating room waiting area by Alpha-Stim fixed at below 200 μA, 0.5 Hz. Ear clips were attached to the ear lobes and the current level was adjusted to below the feeling of a tingling sensation in the ear lobes or feeling dizzy, “just below” 200 µA.
Study Blinding
The investigators were masked to which subjects reviewed CES or were controls.
Outcome Measures
A five point Likert Scale was used to measure anxiety; (1) Strongly Disagree, (2) Disagree, (3) Neither disagree or agree, (4) Agree, and (5) Strongly Agree. A Likert Scale to measure anxiety has established reliability and validity (Davey, 2007).
Results
Subjects
Sixty (60) adults between the ages of 18-65 were subjects in this study. Subjects were waiting for surgery under general anesthesia and met the American Association of Anesthesiology Physical Classification Criteria 1 and 2. Subjects were having orthopedic, gynecological and ear, nose and throat procedures requiring about 2 hours and the surgical procedures had similar risk factors.
Baseline Measurements: Group Equivalence
There were no statistically significant differences at baseline between active CES and sham treatment groups on the outcome anxiety measure. There were no differences in age, gender, height and weight distribution between the two groups. There was no difference in anxiety scores of surgical pre-operative room measurements between the CES and control groups.
Data Analysis
Data were analyzed using t-test to compare the CES and control groups on anxiety scores.
Anxiety
As seen in Figure 1 the CES group had lower anxiety scores on the Likert scale compared to the control group at the endpoint of the study (p < 0.01, d = -.88).
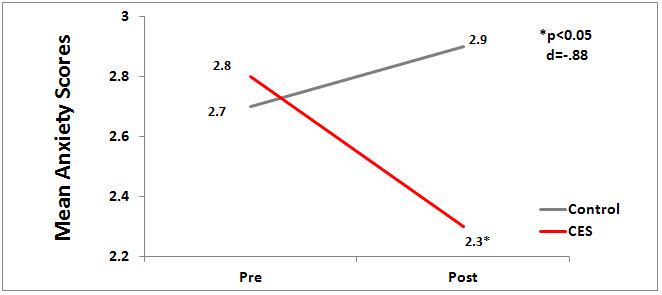
Figure 1. Mean Anxiety Score by Group.
Quality of the Research
Strengths of this study are the randomized controlled clinical trial design; an adequate N of 60 to detect differences between the active and sham groups; and the blinding of the investigators to which subjects received CES treatments. The use of a sham CES device would have increased the strength this study. The findings of this study that CES decreases anxiety are consistent with other RCTs using Alpha-Stim® CES technology.
Author Affiliations
All authors: Department of Anesthesiology and Pain Medicine, Korea University, College of Medicine, Seoul, Korea.
Reference:
Davey HM, Barratt AL, Butow PN, Deeks JJ. A one-item question with a Likert or Visual Analog Scale adequately measured current anxiety. Journal of Clinical Epidemiology. 2007 Apr;60(4):356-60.